The phrase medical-industrial complex can sound dramatic until you watch how modern medicine actually works. Follow the money and you start to see why so many “solutions” in healthcare lead to the same place: more testing, more prescriptions, more specialists, more guidelines, more fear.
In this episode of the A Return to Healing Podcast, Andy and I talk about how medicine got captured. Not by a single villain, but by an entire ecosystem. Pharmaceutical industry influence shows up in the most trusted places, including medical journals, guideline panels, and professional societies. It shapes what gets funded, what gets published, and what gets prescribed.
If you have ever felt like you were being pushed down a pipeline rather than cared for, this is likely why.
Watch the episode on YouTube
If you want more patient-first medicine and less protocol worship, subscribe to the A Return to Healing YouTube channel.
Download the full transcript (PDF) for this podcast episode
The capture is not subtle, it is just normalized
Most people assume the medical system is primarily driven by science. Science matters, but incentives often matter more.
A medical journal relies on advertising revenue. A professional society relies on sponsorship. A guideline panel is filled with experts who have careers tied to a worldview, often with relationships to industry. A university department needs grants. A hospital system needs procedure volume. A politician needs donors.
None of these realities automatically mean corruption. What they do mean is that “neutral medicine” is harder to find than people think. The system’s financial architecture nudges decisions toward more medical activity, and then calls it progress.
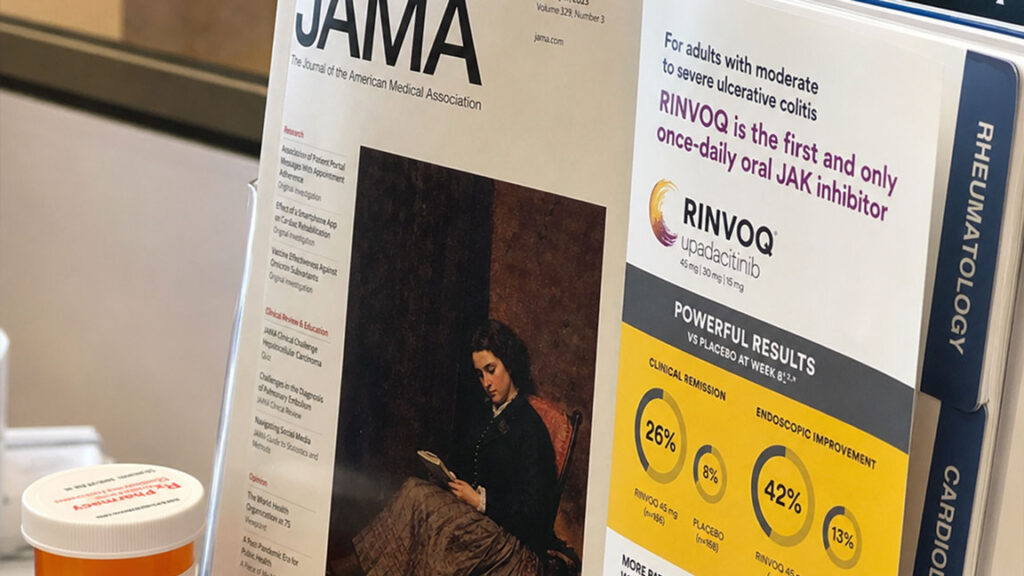
Drug ads in medical journals are not an accident
If a medical journal is funded by pharma advertising, it becomes harder to imagine the journal as an entirely independent referee. That does not mean every paper is fake. It means the culture around what gets amplified, what gets treated as important, and what gets ignored is influenced by money.
The result is not always lies. Sometimes it is imbalance. You hear a lot about drugs and less about the foundational work that makes people healthier but does not create revenue.
Conflicts of interest in medical guidelines create “certainty” where it does not belong
Guidelines are often treated like law in clinical practice. They are not law. They are recommendations written by humans, often based on imperfect evidence, and often influenced by the same forces that influence the rest of medicine.
The most dangerous part of guideline culture is false certainty. The guideline becomes a shield: “I followed the guideline, therefore it was right.” This is one reason the medical-industrial complex spreads so effectively. It creates standardized pathways that are easy to defend and hard to challenge.
You see it everywhere: cholesterol targets, screening rules, “pre” diagnoses, risk calculators, and a long list of numbers that become moral obligations. In a recent podcast episode, we explain how LDL targets keep moving and why ‘lower is better’ can backfire.
Publication bias is how medicine learns the wrong lessons
People assume that “the evidence” means the full record. Often it does not. Studies can be delayed, selectively reported, or never published. That is not a fringe claim. It is a structural problem in how modern research is funded and disseminated.

This matters because guideline panels and clinicians often rely on summaries, meta-analyses, and “what’s accepted.” If the underlying dataset is incomplete, then the conclusions can be confidently wrong.
In the episode of the podcast, we talk about examples where the public story and the full data story did not match. The details differ by drug, but the pattern repeats: big claims, selective evidence, then quiet revisions later.
Lobbying is how the system protects itself
Most patients do not realize how much pharmaceutical industry lobbying shapes policy, payment structures, and regulation. That influence is one reason the same fixes are always promoted. When the only reimbursable solutions are tests and drugs, then the system becomes a test-and-drug machine.
This is also why prevention is talked about constantly and implemented poorly. Real prevention is slow, messy, and not easily monetized. A pill is monetizable.
The most practical tool for patients: “Who paid your expert?”
This is where we give people something concrete. When a doctor or “expert” is aggressively promoting a medication, a screening program, or a guideline target, it is reasonable to ask whether they are financially tied to the industry that benefits.
The ProPublica doctor payments database is one of the easiest public tools for this. You do not need to assume bad intent. You simply need context. Context is what patients are denied most often.
What you can do without becoming cynical
This is not an argument for rejecting medicine. It is an argument for refusing to outsource your judgment.
A useful mindset is this: if a recommendation creates a lifetime of follow-up, repeat testing, and escalating medication without clear improvement in how you live and function, slow down. Ask what outcome it changes. Ask what the absolute benefit is. Ask what the downsides are. Ask what happens if you wait.
If the answer is mostly fear, you are not being cared for. You are being managed.
How we Return to Healing
The antidote to captured medicine is not a new guideline. It is a different model of care.
Relationship-based primary care is slower, more personal, and more honest about uncertainty. It can also do something guidelines cannot: see the whole person. It can weigh values, tradeoffs, and context. That is the kind of care that protects patients from pipelines.
If the medical-industrial complex is built on volume and certainty, then returning to healing is built on judgment and trust.
If this episode made you uncomfortable, that is the point. The medical-industrial complex depends on people not noticing how the incentives work.

Watch the episode, download the transcript, and share it with someone who is overwhelmed by medical decisions and wants a clear framework instead of fear.
→ Watch the episode on YouTube
→ Download the transcript (PDF)
→ Read more from A Return to Healing and explore the framework in our book
Proofread by Dr. Andy Lazris
This post was reviewed for medical clarity and balance. The goal is not cynicism. The goal is to help patients and clinicians recognize incentives, resist fear-based pipelines, and return medicine to patient-first care.
Medical-Industrial Complex FAQ
What is the medical-industrial complex?
It is the network of incentives that connects industry, research, media, professional societies, hospitals, and policy. It tends to reward more tests and prescriptions, even when outcomes do not improve.
Are all guidelines bad?
No. Guidelines can be useful summaries. The problem is treating them like law, ignoring conflicts of interest, and using them to replace individualized care.
Why do drug ads show up in medical journals and media?
Advertising money is a major revenue source. That can shape what gets emphasized and what stays invisible.
What is publication bias?
It is the selective publication or reporting of research results, which can distort the medical evidence base and create false confidence.
How can I check if a doctor receives money from drug companies?
Use public databases like ProPublica’s doctor payments search or Open Payments. Context matters.